What if your bloating has nothing to do with food?
Many people spend years chasing food sensitivities, convinced that one more elimination diet will finally solve their digestive problems. But gastroenterology dietitian Tamara Duker Freuman says some of the most stubborn cases of bloating are caused by something far less obvious: retained stool, trapped gas, and pelvic floor dysfunction. Here are the signs your digestive symptoms may have a different explanation.
For a dietitian employed in a gastroenterology practice, the low FODMAP diet is easily one of the most effective tools I have for managing a variety of digestive symptoms, from bloating and abdominal pain to excess gas and diarrhea.
For people with Irritable Bowel Syndrome (IBS) in particular, the low FODMAP diet has a very high success rate: some 70% of individuals experience marked improvement in their symptoms on the diet.
And once the Elimination Phase offers ‘proof of concept’ that your symptoms are worsened by one or more high FODMAP foods, you can proceed with systematic challenges to identify which families of FODMAP—and in what quantities—aggravate you personally, such that you need only restrict your diet of those foods that trigger symptoms.
When The Low FODMAP Diet Is Not Enough
Stool Burden and the Low FODMAP Diet
While a dietary intervention that benefits 70% of people with IBS seems like a home run, it does beg the question: what if you’re among the minority of people who don’t experience adequate relief from it? Where does that leave you?
There are many reasons why someone with chronic abdominal bloating, pain or bowel irregularity may not feel relief on a low FODMAP diet.
But in my clinical experience, there is one that’s hands down more common than the rest: a high stool burden. As in, being backed up. Or to put it bluntly: being quite literally full of sh*t.
Yes, You Can Be Full Of Sh*t
You can be full of sh*t, or as we like to say, FOS. Because when your colon is packed full of stool—and the pockets of trapped gas that often get stuck behind that stool—you can eliminate all the FODMAPs in the world and still be a distended, bloated, painful, gassy, miserable mess.
People who have historically tended toward the constipated side often aren’t surprised to hear me tell them that their lack of response to the low FODMAP diet could suggest a high stool burden.
They’ve long recognized that even low FODMAP foods that are high in fiber—like salads, popcorn, peanuts, seeds and berries—seem to feel a whole lot worse than low fiber alternatives like eggs, meat, peanut butter, bread and rice.
They also recognize that the severity of their bloating improves somewhat when they are able to move their bowels well—and even more so if they are blessed with a bout of diarrhea that cleans them out more than usual. But even after a great poop, the bloating starts to build again within hours, once they resume eating.
However, I have a significant number of patients who are quite surprised to learn that they may be FOS. These are people who may move their bowels daily—sometimes even more than once.
‘How can I be constipated when I poop daily?’ they often ask me.
The answer really comes down to inputs versus outputs: how much fiber do you consume daily, and how does this compare to the amount of stool you eliminate daily? If more is going in than is coming out on a consistent basis, you can easily become backed up without even realizing it.
What Goes In Should Be Coming Out – But Doesn’t Always

It’s not abnormal for a patient who follows a whole foods/plant-heavy diet to need to move their bowels 3-4 times per day (and occasionally, even more often!)
Similarly, many of my patients who follow various forms of elimination diets—whether grain free , Whole 30 or low carb—wind up eating a whole lot of vegetables and nuts to compensate for the missing food groups in their diet. These diets tend to be very high in fiber—which is objectively health-promoting, but not necessarily well-tolerated by all. Since fiber is indigestible by nature, all that goes in must come out.
Some signs that you might be FOS–even if you move your bowels daily—include:
- You wake most days mildly bloated/distended, and it keeps building as the day progresses
- You end every day visibly distended and often uncomfortable, in pain and/or farting a lot, no matter what you eat
- Elimination diets have had only a modest impact on your symptoms
- You may have the urge to move your bowels multiple times per day, but only tiny little bits come out (and sometimes, nothing comes out at all)
- Even when you do go, you may feel like your bowel movements are incomplete—that there’s more in there that needs to come out but can’t
- Your bloating and distension is worse after a large volume or high fiber meal, and more modest after liquid meals, small portions or low fiber meals
Save this article
We Can Prove You Are FOS
If you suspect that you may be carrying around a high stool burden, a doctor can verify this with basic imaging: X-rays, ultrasounds or CT scans are all able to capture the amount of retained stool in your colon. A gastroenterologist can often tell just by looking at and palpating (pressing on) your abdomen. The question is: what to do about it once its confirmed?
If you’re lucky, resolving a case of “backed up bloating” (as I like to call it) may just require giving your bowels a bit of a nudge with some gentle over-the-counter support from osmotic laxatives like magnesium or Polyethylene glycol 3350 (MiraLAX), stimulant laxatives like senna or bisacodyl (Dulcolax), or some combination thereof.
Often, scaling back a bit on your fiber intake is helpful as well. No need to add flax AND chia to your already fibrous oatmeal with berries. Have a half soup and half salad for your plant-based lunch instead of a giant entrée salad. Get your nut fix from nut butters rather than raw, whole almonds. Eat more of your veggies cooked as opposed to raw. In my practice, I refer to this as a “GI Gentle” diet.
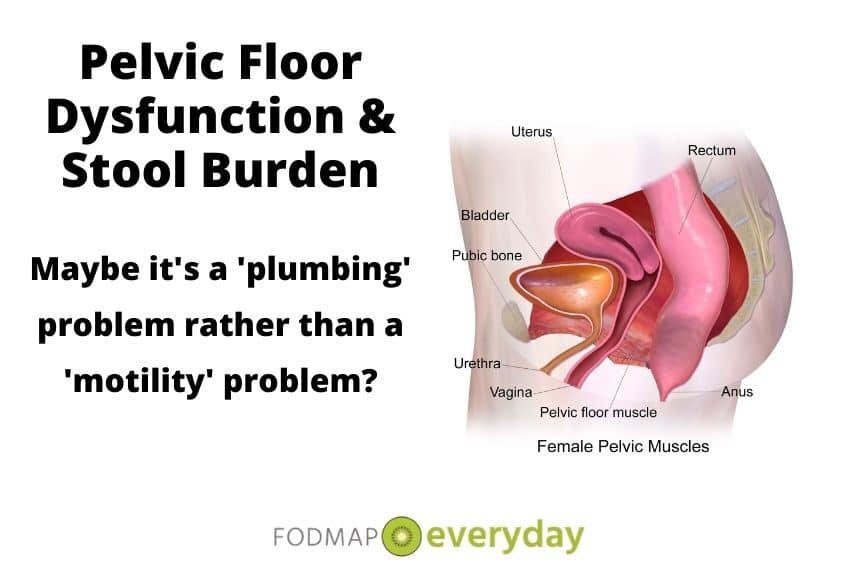
Let’s Talk Pelvic Floor Dysfunction (PFD)
But if you struggle to move your bowels better even with the support of an assertive bowel regimen, it may be worth considering the possibility of pelvic floor dysfunction (PFD).
PFD is a term that refers to a variety of functional problems with the nerves and muscles that support the organs in your pelvic region, and that must coordinate in a specific way to enable you to move your bowels completely and easily. (I tend to think of it as ‘plumbing problem,’ as opposed to a motility problem.).
For a condition you may not ever even have heard of, PFD is surprisingly common. The best estimates I’ve seen suggest that it affects about 17% of women and 5% of men, but prevalence increases after age 40.
PFD is also much higher among women who have given birth—and especially among women who have given birth vaginally. Among people who experience chronic constipation, PFD is a pretty common culprit, responsible for an estimated 30-40% of cases.
In my clinical practice, I have observed that certain patients seem especially prone to being affected by PFD. These include people with histories of anorexia, emotional or sexual trauma; anxiety; “holding it in” as children (fear of moving their bowels at school or in toilets other than those in their own homes); and even those who have formal training as ballet dancers.
However, I’m not aware of any research studies to have quantified whether there is indeed an increased risk among people in these groups that support my subjective observations.
PFD Is Not Just One Thing
There are different types of PFD, and they are, in turn, treated differently. One type of PFD, called dyssynergic defecation, is generally treated with a specific type of pelvic floor physical therapy coupled with biofeedback, which helps “retrain” the nerves and muscles associated with pooping so they can coordinate properly again. A pelvic floor physical therapist might also teach you different toileting positions and breathing techniques to help you evacuate more effectively.
A type of PFD in which the anal sphincter is not relaxing properly may be treated with Botox injections or rectal valium suppositories.
PFD caused by a rectocele, which is a weakening of the muscular wall separating a woman’s vagina and her rectum, can be treated in a variety of non-invasive ways—from bulking fiber supplements to physical therapy to small support devices called pessaries. Severe cases can be repaired surgically.
Given the variation in types of PFD and appropriate treatments, one can appreciate how important diagnostic testing would be in order to clarify the nature of the issue.
The Takeaway
It’s pretty common for people with chronic bloating and other GI issues to automatically assume that their symptoms are a result of a food intolerance or sensitivity. But the relatively common occurrence of a high stool burden as a culprit for chronic bloating is an important reminder that this is not always the case.
By continuing to eliminate more and more foods in a quest to identify an elusive ‘trigger food’ that may not exist, you may find yourself on a fruitless quest for an answer you won’t find… and destroying your relationship with food and eating in the process.
If you continue to struggle with painful bloating and visible distension despite a rigorous trial of the low FODMAP diet, or other commonly recommended dietary eliminations, consider whether you might actually just be FOS. (Rest assured that you’re in excellent company if you are, and we will still love you no matter what). Once properly diagnosed, most causes of a high stool burden are treatable through some combination of fiber modification, medication, physical therapy and/or biofeedback.
Want to learn more about Fiber and IBS? Check out our article here or download this 23 page e-book for 99 cents.
You might also enjoy reading our article, The Scoop on Increasing Your Ability to Poop: Strategies for Alleviating Constipation.
Read All Of Tamara’s Articles:
- What Conventional Wisdom Gets Wrong About Bloating
- Timing of Digestive Symptoms: What It Means
- What Is Leaky Gut Syndrome?
- Are You Full of Sh*t? Stool Burden and the Low FODMAP Diet
- Everything You Want to Know About Farting*
- 5 Reasons to Skip Gut Microbiome Testing – For Now
- Exclusive Interview with Dietitian Tamara Duker Freuman
- Q & A With The Author Of “Regular, The Ultimate Guide to Taming Unruly Bowels and Achieving Inner Peace”








How do you get diagnosed for FOS type issues?
Working with a good RD, like Tamara! You can reach her via her website the Bloated Belly Whisperer.. She is smart, funny and knows sh*t when she sees it:)
As the article explains, your doctor can order imaging tests to evaluate your stool burden.
Hi. Excellent Article. I am a registered dietitian that works with an Acupuncture physician in Jupiter, Florida .I have also found that acupuncture and Chinese Medicine can be a useful therapy for patients experiencing this along with nutrition therapy.
Hi. This article is about ME! I am in the latter stages of elimination diet, test, retest. I cannot eat more than 20g per day of fiber and still eat enough food to achieve my normal 1600-1800 calories without feeling full and bloated. I am not a big eater. I am eating very healthy most of the time and rarely exceed 1650 calories per day. I walk four miles every day and drink lots of water. I weigh 155 lbs and am a 5’9″ male. I am full of fiber because I keep being told that is the answer to resolving my slow motility and IT DOESN’T! I can move gas most of the time but not much else as. Everything in this article describes my situation. I am 73 years old and have been struggling with gut issues most of my adult life without any help from the medical world until I encountered a wonderful young gastroenterologist who has been fantastic. I will be in contact. THANK YOU!!!!
It is Never too late to get better! We are so glad you are in our community and this spoke to you. Tamara is amazing and available for consult, if you would like to reach out to her via her site: https://www.thebloatedbellywhisperer.com. We also highly recommend her book, The Boated Belly Whisperer. Amongst the group of us we know a lot of FOS people who are finally getting the help they have so desperately needed.
Yes, this is me too. Like you I can’t eat more that 20 gms of fiber a day but try telling that to a gastro doc. They seem to think fiber is the answer to everything. The low FODMAP helped me. I think my problem is due to a metabolic disorder. My mitochondria just don’t make enough energy to power my muscles. I have to use a wheelchair because of this. Since the digestive system is a muscle I am guessing this is part of my problem.
Maybe share this with your medical team. Anything that can help, right? We have to advocate for ourselves and sometimes we do know things about our own bodies that we have to point out to the MDs. I have no idea if your doctors will think this is pertinent to you situation, but it doesn’t hurt to have the conversation.
Does anyone get short of breathe being so bloated. Nauseated pain in chest right side. I rarely go. I’m getting tube test rectum test and capsule swallow test.
Its not unheard of. If there’s a lot of gas in the GI tract and/or the colon is very full of stool, there can be pressure on the diaphragm that may make it feel hard to fill the lungs with air. Imaging studies that visualize the gas/stool burden can verify whether this is the case, though the tests you describe will be geared at understanding why you may be full of gas, stool or both.
Hello! I have IBS-C. I am very sensitive to fructans. I can tolerate a slice of regular wheat bread or 1 cup of pasta. In order to not stack, I rely on low Fodmap flours. Unfortunately, most prepackaged foods and flours are either heavily processed and or mainly made with rice flours all of which add to my constipation.
Everyone raves about Udi products
Their Soft White Delicous bread made me feel awful. All of the different gums, modified cellulose( IMO, really terrible for anyone) pea starch and potato starch in addition to rice flours.
I have tolerated Bob’s 1-1, but still have to limit my intake. Rice is binding. Rice is always the go to when you’re sick with diarrhea.
For people like myself with IBS-C and fructan sensitivity what are our best food choices in the way of breads, pasta, snacks, sweets?
I think that rice’s reputation as “binding” really mis-characterizes it’s nature. Rice is NOT constipating insofar as it doesn’t actually SLOW down your GI transit time. In fact, since rice flour is a highly digestible starch with no fiber, it is fully/completely absorbed early on in the small intestine such that there should be minimal to no ‘residue’ leftover to arrive in the colon at all. It’s not going to add to your stool burden when you have constipation. It’s reputation as a good for diarrhea is because it has no fiber and therefore doesn’t aggravate a tendency toward excessive pooping… but it hardly stops diarrhea. Think of rice as more “GI neutral”– shouldn’t help or hurt if you have constipation, shouldn’t help or hurt if you have diarrhea. If you tolerate The Bobs 1:1 or other rice based products in moderation, then I see no reason to avoid them. If you feel starchy foods “add to your constipation,” I wonder whether what you are experiencing is that eating larger amounts of low fiber food in general crowds out portions of fiber-containing foods you need to help you go? Just a though.
And: if you’re looking for a nice bread without fructans, I like the Canyon Bakehouse 7-Grain myself.
Thank you! I think you are onto something about low fiber foods crowding out fiber foods. Yes, in general I feel like all starchy foods bog me down. I believe that my body has an issue with all grains/starches, even lowFodmap. Since posting my questions and reviewing my food logs, I do believe I have other issues playing into my GI problems other than Fodmaps. I’m going to discuss with my dietitian(she is part of this group:)
I started the lowFodmap diet in August/ September. In the beginning I tried gf products prepackaged and flour blends. Each time felt bloated and backed up. So I backed off, ate no prepackaged gf products, ate sourdough bread and kept to brown rice pasta and would treat myself to an oat cookie or oat bread from time to time. I felt better.
At Thanksgiving reintroduced Bob’s 1-1 to make pies. Month of December made different cookies and tried pizza crust and Udis. Still not feeling great at all and feel worse than if I eat AP flour. If I’m being completely honest with myself, gf flours are not good for me even in moderation. Gums are another big problem for me all of which are in gf flours. I’m finding also the less processed foods I eat the better off I am. I’ve done well with Spelt Sourdough bread from Berlin Bakery, Ebans oat bread and Rustik sourdough all of which have a very short ingredients list.
I feel like I’ve come far, but still have much to learn. This diet can be so confusing at times and so scientific that it hurts my brain 🤣 At least I’m making progress.
I just ordered your book and look forward to reading it!
Hi Kim, Dédé here…just wanted to thank you for writing. Isn’t Tamara amazing? She is brilliant and has such a compassionate way of writing and explaining. It is a learning curve for us all!
❤️ I think you all are amazing in this group! I LOVE this website! Such a valuable resource. After 52 years of dealing with IBS-C, I’m finally getting answers as to WHY and learning how to keep myself healthy. My quality of life has improved greatly. Keep up the great work!!
Kim, thank you for being so engaged. We do the work for folks like you (and me)! Happy New Year.
Oh, my, I am about dying here! I have been constipated for the greater part of my 66 years, starting when I was a baby. That was back when such a thing was called “Chronic Spastic Diarrhea.” One of my favorite definitions was in a medical book that commented that “For reasons we do not understand, the bowels choose to retain fecal material and roll it into small hard balls that are difficult to evacuate.” My mother described it as “bunny turds.” Anyone relate to this?
Then when I was in my 20, I was at my gyn-ob for a check up. The doc is palpating my innards and asks me if I have bowel movement. I told him that I was usually a bit constipated and if I managed to go 3 times a week, I thought it was about normal for me. Now my doc was a very sweet mild mannered man who probably blushed every time he had to check out girl parts, but he was also very thorough and scientific, so it startled me a bit that he told me that I could probably lose 5 lbs if I could move it all out. He said that I was “fully impacted with fecal material!!”
At that point, I lost it and just roared with laughter. I asked him if he was diagnosing me as being “full of shit!” He wouldn’t quite say the words but agreed that he was pretty much saying that! I still laugh when I think of how I have an official medical diagnosis of being FOS!!
I have been doing FODMAP, along with low acid, for over a year now. I still get constipated. Three times a week is still about the best I can do. I get tired of feeling like I need help to go but sometimes I need to take something else.
I was laughing reading this…with you (promise), not at you. We get it; we really do. And it is so unfortunate that we hear from many people that their GI issues have been decades long issues, just as you described. Have you worked with a Registered Dietitian? A RD could work with you on your particular FOS presentation.