What Is IBS?
An estimated 10 to 15 percent of the worldwide population lives with irritable bowel syndrome (IBS), a chronic Disorder of Gut-Brain Interaction (DGBI) that affects the large intestine.
IBS can cause abdominal pain, diarrhea (IBS-D), constipation (IBS-C), alternating episodes of both diarrhea and constipation (IBS-M), or symptoms that do not fit neatly into one category (IBS-U, or unclassified IBS). Many people also experience bloating, pressure, cramping, fullness, or abdominal discomfort. Changes in bowel habits and stool appearance are also common. Not every person with IBS experiences all symptoms, and symptom patterns can vary widely from person to person.
For many years, IBS was classified as a “functional gastrointestinal disorder,” meaning symptoms occurred without visible structural abnormalities on routine testing. However, this terminology has increasingly fallen out of favor.
Today, IBS is classified as a Disorder of Gut-Brain Interaction (DGBI), a term that better reflects current scientific understanding of the the many complex interactions.
Research has now shown that IBS involves complex interactions among the gut microbiome, nervous system, immune function, gastrointestinal motility, and communication between the gut and brain. Motility refers to the movement of food and waste through the digestive tract.
In people with IBS, these movements may occur too quickly, too slowly, or in a dysregulated way, contributing to symptoms such as diarrhea, constipation, cramping, bloating, and abdominal discomfort.
There is even something called “high stool burden”. Bloating, gassiness, bowel urgency, and mucus in the stool are also common in IBS. Weight loss or weight gain can be a side effect of IBS.
What Causes IBS?
Despite its prevalence, the exact cause of IBS is still unknown, and we don’t have diagnostic tests for it like we do for celiac disease and inflammatory bowel disease (IBD). Still, there has never been more interest in understanding and treating this complex disorder.
The most promising area of IBS research concerns the “gut-brain axis,” which is a shorthand term for the way the brain and gastrointestinal tract communicate. If you’ve ever had “butterflies in your stomach” or an urgent need for the bathroom before an exciting or upsetting event you’ve experienced the gut-brain axis in action.
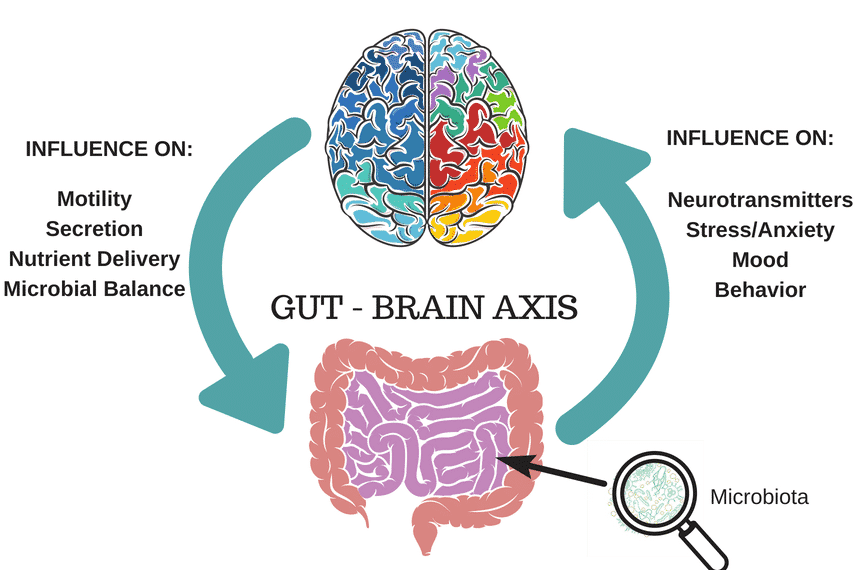
The important thing to understand is that gut-brain axis is a two-way street, with the brain influencing how the gut functions and the gut modulating how the brain functions.
Researchers suspect that disruptions in this pathway cause the intestinal motility problems and increased sensitivity that lead to classic IBS symptoms of diarrhea, constipation, and pain. Furthermore, they suggest that gut bacteria –– the gut microbiome –– play a big part in causing brain and gastrointestinal tract to miscommunicate in the first place.
How Is IBS Diagnosed?
There is no formal test for IBS that is widely used or particularly reliable*; IBS is typically diagnosed based on symptoms, after certain tests may be done which screen for diseases and conditions that present same or similar symptoms. It is very important that you do not self-diagnose. Please read our article, IBS: Step-by-Step Guide from Diagnosis to Symptom Free Living, for more information.
*(Though there is no universally applicable diagnostic tool for all IBS forms, there is a relatively new, commercially-available antibody blood test called IBS-Smart. This test measures biomarkers associated with IBS-D and IBS-M, which may be elevated following infectious gastroenteritis and presents a potential diagnostic option for post-infectious IBS-D and IBS-M. As always, consult with your trusted health professional to learn more if they believe this may be a useful tool in your diagnosis Please read our previously published article that discusses this test for more information, and discuss the advantages and limitations with your medical team.)
For a more thorough look at IBS diagnosis, please read How Is IBS Diagnosed?
Gastroenterologists Can Diagnose
A gastroenterologist (GI) or MD should first review your full medical history and perform a physical exam, then will most likely order blood, urine, and/or stool tests and screen you for celiac disease. Depending on your symptoms, they might also screen you for IBD (inflammatory bowel disease), Crohn’s, diverticulitis and/or endometriosis.
A colonoscopy might be recommended, and some doctors will order X-rays or CT scans, lactose-intolerance tests and/or breath tests for SIBO.
Gastroenterologist should also use the Rome V Criteria (the Rome Foundation creates guidelines for diagnosing IBS). GIs are more likely to be familiar with this criteria than your General Practitioner.
A formal IBS diagnosis will be given when other medical issues are ruled out and your symptoms match those that are indicative of IBS, such as those presented in the Rome V criteria.
A formal IBS diagnosis will be given when other medical issues are ruled out and your symptoms match those that are indicative of IBS, such as those presented in the Rome V criteria.
How IBS Diagnosis Has Changed Under Rome V
The release of Rome V in 2026 marked one of the biggest shifts in IBS diagnosis in more than a decade. Earlier Rome criteria relied heavily on rigid symptom definitions designed largely for research studies. Rome V now separates research criteria from clinical criteria, giving healthcare providers more flexibility when diagnosing patients in real-world settings.
One of the most important changes is that Rome V once again recognizes abdominal discomfort alongside abdominal pain as part of IBS diagnosis. Rome IV had removed “discomfort” and required abdominal pain at least once per week, which many clinicians felt excluded patients who clearly had IBS symptoms such as bloating, pressure, cramping, fullness, or generalized discomfort.
Rome V also lowers the symptom threshold, meaning some patients who previously did not fully meet Rome IV criteria may now receive an IBS diagnosis sooner and gain earlier access to treatment and support.
The updated framework also continues moving away from the outdated idea that IBS is “all in someone’s head.” IBS is now understood as a complex Disorder of Gut-Brain Interaction involving the nervous system, gut microbiome, immune function, intestinal motility, and communication between the gut and brain.
Gut Microbial Composition
A point of interest: Recent scientific studies have shown that certain types of microbes are found in the gut of those who are more likely to have IBS; for instance, gammaproteobacteria seem to be in greater abundance in both children and adults who have IBS. Other pathogens, such as Clostridioides difficile, may also be contributing to IBS symptoms. Researchers are hopeful that these findings will aid in diagnostic and therapeutic approaches. In the future it might be possible to make very specific recommendations for individuals, for probiotics and prebiotics for instance, based on their unique gut microbe presentation.
The low FODMAP diet is one such approach that can alter microbial composition in a positive way for some of us with IBS.
IBS is now understood as a complex Disorder of Gut-Brain Interaction involving the nervous system, gut microbiome, immune function, intestinal motility, and communication between the gut and brain.
How Is IBS Treated?
It’s very frustrating to hear that the cause, much less the “cure”, for such a common condition is still unknown, but we do have more ways of treating IBS than ever before. These interventions generally fall into three categories: dietary, pharmaceutical, and psychological.
- Dietary: The premier dietary approach for IBS ––the low FODMAP diet – has been shown to provide significant symptom relief in 75 percent of people who try it. That’s a remarkable statistic. It’s also why our goal at FODMAP Everyday® is to help you understand and incorporate the low FODMAP diet into your everyday life. You can read more about the diet here, and then start putting it into practice with our delicious low FODMAP diet recipes.
- Pharmaceutical: Medications for IBS are *numerous but they often target only one of the predominant symptoms which is problematic if you suffer from two or more. Another drawback to using drugs for IBS is the potential for side effects.
- Psychological: The most well researched psychological interventions for IBS are cognitive behavioral therapy (CBT) and gut-directed hypnosis. These are particularly helpful for people whose symptoms are exacerbated by stress. Both CBT and gut-directed hypnosis have success rates that surpass many medications but they also require a greater time and emotional commitment.
*Alternately https://emedicine.medscape.com/article/180389-medication
Diet Is Now Recognized as a Core Part of IBS Management
One of the most meaningful changes reflected in Rome V is the formal recognition that dietary therapy is a central part of evidence-based IBS management. For years, many patients were told their symptoms were primarily caused by stress or anxiety, despite growing research showing that food can significantly affect IBS symptoms for many people.
Today, dietary approaches such as the low FODMAP diet are recognized alongside medications, behavioral therapies, gut-directed hypnotherapy, and other multidisciplinary treatments. Rome V also reinforces the importance of individualized care and working with a dietitian trained in digestive health whenever possible.
This shift reflects how much scientific understanding of IBS has evolved. Researchers now recognize that IBS involves complex interactions among the gut microbiome, nervous system, immune function, gastrointestinal motility, and the gut-brain axis.
What Makes IBS Symptoms Worse?
While there is no one thing – food or otherwise – that creates IBS, there are many things that can trigger or exacerbate symptoms. These include, but are not limited to: high FODMAP foods, dairy products, lactose intolerance, depression, stress, anxiety, spicy food, caffeine, prescription and over-the-counter medicines, supplements, digestive tract infections, to name a few.
To read how others handle their IBS flares, check out our article, How To Relieve An IBS Attack.
Who Should Be on Your IBS Care Team?
Because IBS is now understood as a Disorder of Gut-Brain Interaction (DGBI), many people benefit from a multidisciplinary approach to care rather than relying on a single provider. Depending on your symptoms and their severity, your IBS care team may include a gastroenterologist, primary care physician, dietitian trained in digestive health, pelvic floor physical therapist, psychologist or therapist familiar with gut-brain therapies, and sometimes additional specialists.
A gastroenterologist can help evaluate symptoms, rule out other digestive diseases, and guide medical treatment. A dietitian trained in IBS and the low FODMAP diet can help identify food triggers while maintaining nutritional adequacy and avoiding unnecessary restriction. Mental health professionals experienced in gut-directed cognitive behavioral therapy, hypnotherapy, or stress management techniques may also play an important role, since the gut and brain are closely connected. Nerva is a fantastic app-based gut-directed hypnotherapy program.
Some people with constipation, incomplete evacuation, or pelvic pain may also benefit from working with a pelvic floor physical therapist. The goal is not simply symptom suppression, but improving overall quality of life through individualized, evidence-based care.
The Takeaway
It is possible to live a pain-free and symptom-free life with IBS by using the management techniques that work for you. In other words, the long term outlook is good!
Step #1 is getting an accurate diagnosis from a medical doctor or gastroenterologist, and then consider working with a Registered Dietitian, pelvic floor physical therapist, psychologist or therapist familiar with gut-brain therapies, and/or sometimes additional specialists.
Your GI might suggest the low FODMAP diet, in which case FODMAP Everyday® will be of immense help. The low FODMAP diet has been clinically proven to provide relief for about 75% of the 1 in 7 people worldwide who are diagnosed with IBS. Although a doctor might not mention this, the diet is meant to be undertaken along with a RD.
Here at FODMAP Everyday® we have 1500+ recipes and hundreds of evidence-based articles written by Monash University trained dietitians (Monash researchers developed the diet).
Dédé Wilson, our lead recipe developer, is Monash University dietitian trained as well, and also FODMAP Friendly Accredited as a FODMAP educator – as is FODMAP Everyday®. So whether you need information on IBS, the low-FODMAP diet, gut-friendly recipes, or a community of others experiencing GI distress, you have landed in the right place.
Additional Sources and References:
From FODMAP Everyday®:
- The Role Of The Dietitian vs. The Gastroenterologist
- What Is IBS?
- Deadly Diseases That Mimic IBS
- Understanding the Overlap Between IBS & Anxiety
- Have IBS? Top Reasons To Work With A Dietitian
- How To Choose A Dietitian
- Dietitians & Nutritionists: What’s The Difference?
- Patient Dos And Don’ts For A Great Telehealth Appointment
Other:
- Rome V Diagnostic Criteria
- IBS Overview – National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
- Celiac Disease Diagnosis – NIDDK