Welcome to the wild ride that is IBS-M.
For those who aren’t yet familiar with this charming condition, IBS-M stands for Irritable Bowel Syndrome with mixed bowel habits, meaning you alternate from constipation to diarrhea.
More on the symptoms of IBS Mixed, how it’s diagnosed, and what to do about it will come shortly-don’t worry!
But first thing’s first (just in case the following news flew under your radar like an F-117 Nighthawk)…
- IBS Defined
- Back To Why We Are Here: IBS-M
- The Gut-Brain Interaction
- Diet & IBS-M
- Medications: What to Ask Your Doctor
- Supplements for IBS-M: Game Changing, If Done Right
- A Word of Caution
- Handling the Extremes: Constipation & Diarrhea Days
- What About SIBO & IMO When It Comes to IBS-M?
- Other Issues That Can Look Like IBS-M, But They Ain’t IBS-M
- The IBS-M Recap
IBS Defined

In the past, Irritable Bowel Syndrome (IBS) was described as a type of “functional gastrointestinal disorder”- a set of symptoms that didn’t seem to have an organic cause or reliable testing to clearly diagnose.
But that has changed.
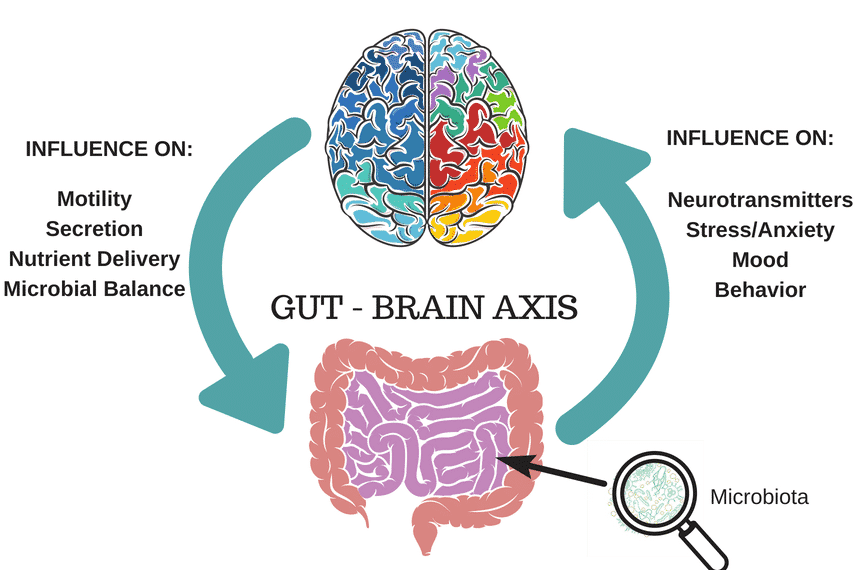
IBS is now formally recognized as one of more than 27 disorders of gut-brain interaction (DGBI).
What the heckin’ heck does that mean?
Simply put, it means that the root cause of IBS is linked to the functioning (or in this case, the miscommunication) of the gut-brain axis.
Like many disorders of gut-brain interaction (DGBI’s) diagnoses, these can come with:
- Irregular speeds at which food moves through the gut: Either too slow, or too fast, which can lead to constipation or diarrhea, respectively. In the case of IBS-M, you get both delights.
- These irregularities in gut speed are called motility disturbances, and/or “dysmotility”.
- Changes in the types, numbers and patterns of diversity of our “gut bugs”: This can have a huge effect on all sorts of “gutty” things, like how fast or slow the gut moves our food and gas along, level of abdominal pain experienced (see next bullet), the likelihood of having additional suspected food intolerances (like histamines and/or food chemicals, and even starches and certain sugars like sucrose and lactose).
- This is referred to as an altered gut microbiota, and/or “dysbiosis”.
- How sensitive our gut lining is to stretching and/or pressure of its contents like food, gas and poop, and how the brain may be misinterpreting these signals from the gut (usually amplifying them inappropriately. Not cool brain. Not cool at all).
- In gut geek talk, this is known as “visceral hypersensitivity”
- Inappropriate responses back and forth from gut to brain via the vagus nerve. Interestingly, lots of this scrambled signalling can be influenced by those “gut bugs”. Not only that, but the opposite is also true: Our nervous system (in particular when we spend too much time in our stress response- when we’re in “fight, flight, freeze, fawn”) can also influence how our “gut bugs” behave right back.
- In science lingo- this is referred to as “alterations of the gut-brain axis”.
- Other “layers” to each person’s individual constellation of IBS symptoms.
Ok, now that we’ve defined what a DGBI is, and that irritable bowel syndrome is now considered a DGBI, for anyone who is a newcomer here, let’s run down some basics as to the diagnostic steps that (should) come before arriving at an IBS diagnosis, shall we?
Before IBS is diagnosed by your Doctor or Gastroenterologist, there are tests that should be done to rule out some of the bad, the ugly and the downright dangerous conditions that may have overlapping symptoms similar to IBS.
Once this is done and dusted (and ideally all results are negative), the Rome IV criteria is then applied- and it goes like this:
Recurrent abdominal pain on average at least 1 day/week in the last 3 months, associated with two or more of the following *criteria:
- Related to defecation (meaning pain comes when you need to poop, during the poop, and in general one feels better after the poop)
- Associated with a change in frequency of stool (meaning poops are coming too fast and furious, or poops ghost you several days of the week)
- Associated with a change in form (basically poops get either too soft, mushy or watery, or they get too hard and lumpy)
- In the case of what we are here to talk about today, IBS-M usually rocks out both point 2 and 3.
*PS: The criteria above needs to be fulfilled for the last 3 months, with symptom onset at least 6 months prior to diagnosis (meaning it came, and it doesn’t seem to be going away anytime soon, as opposed to a gut issue that’s temporary, or “acute”, for example, like food borne illnesses, parasitic infections, or that lovely Noro treat your kids brought home last fall).
Nothing “a-cute” about that.
Sorry, I had to.
In normal terms?
Basically, IBS is described by a combination of recurrent abdominal pain, typically 4-12 hours after eating, pain before, during, and/or after pooping, and changes in bowel habits (constipation, diarrhea or back and forth between the two).
Then comes assigning you a subtype of IBS. This is ideal, because knowing your IBS subtype can increase your ability to source better information and care, like my free IBS-M Mini Guide.
There are four IBS subtypes: Diarrhea, Constipation, Mixed, and Unclassified.
You meet the criteria for IBS-M if:
- More than 25% of your abnormal poops are loose or watery (Type 6 or 7 for those keeping track)
AND
- More than 25% of your abnormal poops are hard, dry and/or lumpy (Type 1 or 2).
Before we begin, it is important to note that after diagnosis by a medical doctor, working with a Registered Dietitian (RD) who is a virtuoso in the domain of IBS/gut health is a critical step to begin your road to “Aaahhh…that’s much better”.
Back To Why We Are Here: IBS-M

The cycling between constipation and diarrhea, the bloating, gas, and abdominal pain—it’s a real party.
So, let’s dive into some practical, science-backed strategies to help you manage this thrill ride of a condition.
First off, there is nothing more important to understand about IBS-M than this:
IBS Mixed is rooted in constipation (not diarrhea)!
More on why that is so critical later.
Let’s look at a week in the life of someone with IBS-M first.
The typical scenario I see in my practice looks something like this:
- First, one to three days of constipation is experienced
- During this time, feelings of bloating, abdominal pain and pressure usually start to increase
- Then, over a period of one or two days following the constipation days, several loose bowel movements move through in fairly large volumes- often with mucho urgency and “explosiveness” as my clients tend to describe it
- The diarrhea in this case tends to be more of a result of the “dam of poop breaking” as opposed to diarrhea due to the gut simply moving too fast making looser, waterlogged poops in the case of IBS-D (this is my joy of a subtype by the way).
The Gut-Brain Interaction
It’s important that we re-emphasize that IBS is now classified as a disorder of the gut-brain interaction.
Effective treatment options should look to target the root cause of this underlying constipation-followed-by-diarrhea gong show.
Often it’s the oversensitive nerves in your gut and those faulty signals of the gut-brain axis causing the gut to move too slow (or too fast).
Gut-directed hypnotherapy (GDH) such as the Nerva App is literally magic at this, and unlike medication or diets, the effects can last long term.
Fun fact: GHD is “subtype agnostic” (a fancy way to say that it doesn’t care which subtype you are- its likely equally effective across all IBS subtypes).
Translation: It can address IBS symptoms whether you are an IBS-D, C, M, or U.
Huzzah!
Diet & IBS-M
There are, of course, other explanations for why the IBS-M gut is rooted in constipation, like the health of one’s good ol’ pelvic floor, conditions that affect connective tissue like hypermobile EDS, and certain gut microbe factors like Intestinal Methanogen Overgrowth (IMO), just to name a few.
But, for all intents and purposes, let’s say your case is “straight up IBS-M” and none of the above extra layers to your IBS-M story.
The Low FODMAP Diet: Your New Best Frenemy
It would make sense if you’re already aware of the Low FODMAP Diet considering the website you’re on, but let’s give this a quick tickle, shall we?
One potential dietary strategy to explore is the Low FODMAP Diet which reduces a certain subset of rapidly fermentable carbohydrates. More on the exact details of Low FODMAP here.
This diet isn’t for the faint of heart, but it can work wonders for reducing symptoms like bloating, abdominal pain, etc.
Keep in mind that the full Elimination Phase of the Low FODMAP Diet (Phase 1) is not meant to be long term.
Yet… About 50% of those who start the diet get stuck on the Elimination Phase (hence the “frenemy” portmanteau).
I have to restate (now, picture me on bended knee, hands flailing, and dramatically pleading): Find a Registered Dietitian with multiple years of IBS experience to support you through all phases to eventually get to the least restricted diet required for symptoms to remain well managed.
If this proves difficult despite following the Low FODMAP Diet “by the book”, your GI-focused Dietitian may need to then explore the other possible explanations of stubborn symptoms, such as histamine intolerance, SIBO/IMO, and GSID, for example.
Some low FODMAP food examples that might work well for someone with IBS-M (and some perks of each) include:
- Sourdough bread (as long as Celiac Disease has been ruled out)
- Low FODMAP pasta (check out the deal with wheat, gluten & fructans here, and my detailed video on what low FODMAP serving sizes of wheat products look like here)
- Blueberries – Because they’re high in anthocyanins (a type of antioxidant that can help protect against several yucky diseases), and fiber (which is helpful as IBS-M is rooted in constipation)
- Kiwis – Specifically because 2 per day can help on constipation days
- Rice – A gentle source of carbohydrates, especially on diarrhea days
- Carrots – High in beta-carotene, potassium and a soluble fiber called pectin
- Oranges – High in fiber, and also antioxidants like lycopene and vitamin C
- Nutritional yeast – High in B vitamins important for things like energy production
- Lactose free “wet dairy” like milk for those who are lactose intolerant
Conversely, some of these foods that are high FODMAP might not work for you:
- Onion/shallot
- Beans*
- Garlic
- Mushrooms
- Cauliflower
- Lactose containing dairy products (aka “wet dairy” like milk)
- Apples
- Pears
- Pistachios
- Cashews
- Whole grain bread*
*In addition to a high concentration of FODMAPs, foods like beans and whole grains, are high in roughage (“bulky” sorts of fibers).
On paper, when we’re talking about constipation, taking in lots of fiber may seem like a “plus”; however, if someone with IBS-M is experiencing constipation (as again, the condition is rooted in constipation) these foods may feel more troublesome than other, lower roughage foods).
Why?
Because adding lots of fiber to a constipated gut can feel like adding more cars to a traffic jam.
For a sweet little summary of do’s and don’ts of IBS-M , check out my free IBS-M Mini-Guide.
Medications: What to Ask Your Doctor

I’ll give you the bad news first:
Per the ACG guidelines published in 2020, there are no medications specifically recommended only for the IBS-M subtype (unlike IBS-D and IBS-C, where there are medications available).
As of present day (2025) I am still not aware of any that exist, or that are in the making for IBS-M.
Lame, I know.
However, both Monash University and the ACG suggest that Tricyclic Antidepressants (TCAs) might help alleviate “global” IBS symptoms. Chat with your doctor about this option, but buyer beware…
A well documented side effect (and unfortunately there are abundant side effects) of TCAs is constipation (and remember that IBS-M is rooted in constipation).
The magnitude of which can vary across different types of TCAs, as well as the dose (lower doses are usually employed when used specifically to reduce IBS related symptoms as opposed to use as an antidepressant.
Main point: TCA meds may exacerbate the condition for some people with IBS rooted in constipation (IBS-M and IBS-C); have several side effects, but can be helpful for others (in particular for those with IBS Diarrhea and those with abdominal pain).
Keep your Dr. aware of any side effects and ask if there are alternatives, depending on your response to any medication and/or supplement.
One last note: Oftentimes clients with IBS-M will be advised (or will take it upon themselves) to use loperamide to address the diarrhea side of their symptoms.
I have only experienced the use of loperamide in my practice as worsening my IBS-M patients’ constipation-diarrhea cycling as it tends to pop them right back into “constipation mode”- and the cycle just goes on and on.
(See “diarrhea days” for what to consider instead of drugs to gently relieve diarrhea, so that you reduce the chance of being sent back into the rollercoaster bowel drama that’s classic for your subtype.
Remember though my friend, no medication yet has been proven to be as effective or long lasting as gut-directed hypnotherapy, and with fewer risks of side effects, or fewer dietary restrictions.
Supplements for IBS-M: Game Changing, If Done Right
Supplements can be a game-changer. Here are some picks (but always check with your Doctor first!):
Save this article
For improved stool form:
- Soluble fiber: Partially Hydrolyzed Guar Gum (PHGG) or Acacia Senegal on diarrhea days, and
- A “water magnet” like magnesium citrate or PEG when you want to ensure to keep things moving (and thus avoid becoming backed up)! Chat with your Doctor, because certain people, like those with kidney disease, might not be able to safely take either.
- Pro tip: Being proactive with the above two supplements is how the majority of my IBS-M clients break the constipation to diarrhea cycle!
For bloating and increased food freedom: FODMAP-degrading enzymes like FODZYME.
For abdominal pain: Enteric-coated peppermint oil, like IBGard, & herbal tinctures like Iberogast (the latter contains alcohol and herbs that may not be safe in pregnancy, just FYI).
A Word of Caution
If you haven’t had a bowel movement in 5 to 7 days, don’t reach for that fiber supplement just yet.
Consult your doctor to rule out potential risks like obstruction.
IBS-M can sometimes be complicated by underlying issues like Pelvic Floor Dysfunction, slow transit, or it could simply be mainly constipation that is punctuated by diarrhea for other reasons (see more on that next) and therefore not IBS-M at all.
So make sure you have a good team that are compassionately challenging you to explore these options if possible.
Handling the Extremes: Constipation & Diarrhea Days

If you are “in it” with IBS-M, here is a quick flare-up toolkit you can reach for at any time:
On those delightful constipation days:
- Consider upping your intake of coffee. Yep, even decaf can help due to the fact that it contains chlorogenic acid- that stimulates the gut’s muscles to move.
- PS: The whole “avoid coffee” blanket term for IBS is a little silly. It can be an amazing tool for those with IBS-M or IBS-C when your bowels need a little nudge (or a giant shove. I know you’re catching what I’m throwing here)
- Slam water, or peppermint tea, like its going out of style
- Pop 2 kiwi fruit. These are poop powerhouses
- Grab some FODZYME if you have bloating and use it on your meals to help make your food less gas forming for the next day or two
- And don’t forget to move your body – exercise can work wonders; even if it’s the last thing you feel like doing during a flare-up
Conversely, on diarrhea days:
- Consider upping your soluble fiber intake (my go to for diarrhea is Acacia senegal. It forms stool like a gangsta)
- Swap out coffee for peppermint tea.
- Now this is the time to heed the “decrease coffee” pearl of wisdom
- Enjoy “side acts” of “roughagey” foods like salads and smoothies instead of making them the star of your meal.
- Be a pencil and not an eraser though: Add in other foods like white rice, sourdough, and a good source of protein to nourish yourself
- Make time for gentler forms of movement, like a short walk.
- Or if you are couch-ridden, do a Nerva session and get your nervous system “switch” flipped to the parasympathetic setting (your rest and digest mode, as opposed to your sympathetic “fight/flight” mode. That stress isn’t needed right now a-thank you very much)
What About SIBO & IMO When It Comes to IBS-M?

Did you know, like the other subtypes of IBS, with IBS-M you may also be growing excess gut bugs?
‘Tis true.
The gut can have larger than normal numbers of certain gut bugs hanging out along the gut, such as in the small intestine (as in the case of small intestinal bacterial overgrowth, or “SIBO”) and/or large intestine (Intestinal Methanogen Overgrowth or “IMO” can occur in both the large and/or small intestine).
There is also the new and lesser understood Intestinal Methanogen Overproduction, or “ISO” (this bad boy gas is usually correlated with increased diarrhea however).
Why can this turn into a very bloaty problem?
When these certain gut bugs ferment FODMAPs, and produce hydrogen and/or methane gasses, the resulting gases may speed up or slow down the gut (methane gas tends to be the constipating variety), and increase the sensation of bloating and food sensitivities beyond even FODMAPs like sugars and starches…by a lot.
In a nutshell: SIBO and IMO can occur in about 25% of everyone with IBS-M, and can throw a wrench into your otherwise well drawn up IBS-M treatment regime.
The treatment: Antibiotics, or an antibiotic combination, depending on which of the breath gasses were positive on a breath test.
More on SIBO/IMO/ISO here.
Other Issues That Can Look Like IBS-M, But They Ain’t IBS-M
But note: It’s possible to have IBS-M and another “layer” such as a few described below.
Let’s dive into it.
IBS-M is NOT:
Undiagnosed Celiac Disease (or other serious, undiagnosed conditions like IBD)
Head to the Dr. to ensure these aren’t the reasons for your wild bowels, and request a blood test called an IgA-TtG if you’ve not been screened.
And please; don’t restrict gluten until you’ve had this test done – otherwise it may come back falsely negative.
Overflow diarrhea:
Overflow diarrhea is when liquid stool sneaks past a blockage of poop in your intestines.
If your plumbing is a bit blocked – thanks to chronic constipation, fecal impaction, or even nerve issues- you can end up with watery poop, as fresher stool behind the hard stuck stool sneaks its way past from time to time.
The main sign of overflow diarrhea is runny bowel movements that punctuate bouts of constipation, or even small, regular looking poops that don’t add up to the amount of healthy, fiber-full meals someone eats (like less than ⅓ of a cup- that’s 80 mL for the metric lovers)- but with lower volume than what we typically see with IBS-M.
You might also feel some tummy discomfort and bloating with larger or roughage-filled meals like salads, whole grains and beans. Or you may feel like you just “can’t get everything out”.
If you’re experiencing this delightful combo, it’s time to chat with a doctor who can play the role of your personal plumbing inspector.
They’ll look into your medical history and might even order some tests like X-rays to see if your intestines are what we call in the industry as “FOS” (full of stool) or a colonoscopy to figure out what’s blocking your flow.
Constipation (or IBS-C) with a “Layer” of Histamine Intolerance
If you have:
- More random than regular diarrhea episodes
- Diarrhea episodes that are worse/more frequent in Spring and Fall (after the leaves drop)
- Symptoms that seem worse when you eat certain foods like leftovers, aged cheeses, fermented foods like wine, beer, and soy sauce
- A history of copper, zinc or vitamin C deficiency
- Have non-celiac wheat sensitivity
- Been pregnant and your symptoms seemed better
- Followed the low FODMAP Diet for years (but haven’t moved past the initial Elimination Phase)
- And/or are taking medications like verapamil (a blood pressure and angina med), clavulanic acid (used for certain bacterial infections, usually paired with amoxicillin), and isoniazid (used to treat Tuberculosis)
Then you may have a “layer” of histamine intolerance for various reasons.
PS: It’s important to distinguish histamine intolerance from food allergies, which involve an immune response to proteins in food.
Histamine is a compound found in foods like aged cheese, wine, and fermented products. There are other food chemicals (both naturally occurring, and those added during food processing) that can also “liberate” histamine in some individuals too; like salicylates, for instance.
When your body struggles to break down histamine due to a deficiency in the enzyme diamine oxidase (DAO), you may experience a range of symptoms.
Gastrointestinal issues often include bloating, gas, diarrhea, and abdominal pain.
Non-gastrointestinal symptoms can manifest as headaches, skin rashes, nasal congestion, and even palpitations.
Let me tell you a little story about a client of mine.
Gail (name has been changed to protect client anonymity) came to me with a history of chronic constipation, but with “episodes” every 10 days of nausea, vomiting, and bloating which was followed by non-stop diarrhea for hours. These episodes fatigued her for days.
Gail’s Dr. diagnosed her with dumping syndrome (when the stomach empties a meal too rapidly into the small intestine), due to the fact that Gail had surgery on her esophagus and stomach prior to these symptoms arising (and surgeries like hers increased dumping syndrome risk).
But, upon looking at her diet in the 12 hours that preceded her latest flare-up, several high histamine foods were listed, like leftover miso chicken, leftover slow cooked ribs, pickles, and other fermented and high histamine foods (some of which eaten with the purpose to “improve gut health”…because that was what the interweb said to do).
After taking more history (including discussing the pros and cons of trialing a low histamine protocol), we forged ahead, plus added a “water magnet” of magnesium citrate to alleviate her baseline chronic constipation, and 6 weeks of gut directed hypnotherapy to address the potential of a DGBI.
Fast forward to our four week check-in, and the constipation was gone thanks to magnesium citrate, and thanks to subtle, game changing food storage methods to reduce histamine levels in her foods, we avoided what I lovingly refer to as a “histamine tsunami” (an excess build up of histamine in the body where DAO can’t keep up) and the random diarrhea stopped.
To date, there has not been another serious flare-up for Gale since, and what might have seemed like IBS-M had in fact turned out to be chronic constipation with a good ol’ smattering of histamine intolerance!
Constipation (or IBS-C) + a “Layer” of Sugar Intolerance (Sucrose, fructose, lactose, and/or polyols)
If there is one thing I wish I knew about earlier in my career, it would be sucrase-isomaltase deficiency awareness. I’ll get to that gem in a tick.
Another explanation for periods of constipation punctuated by random diarrhea (that don’t quite add up to that 25% rule to be classified as IBS-M) can be intake of certain sugars or sugar alcohols.
Lactose intolerance is usually easily recognized and managed within the IBS space, as most people can pinpoint “wet dairy” as being a potential problem, remove it, and decide if the bloating and diarrhea are gone or not. There is a breath test to detect this as well. Easy peasy.
Sugar alcohol intake (especially excessive sugar alcohol intake) is also usually pretty easy to spot when someone who is classically constipated all of a sudden explodes with diarrhea, say, after eating a large portion of a “No Sugar Added” treats like chocolate sweetened with maltitol, or sorbitol syrup…
Oooh that last one got me good a few years back after eating a fair amount of a popular chocolate peppermint bar, and it wasn’t even labeled “No Sugar Added”!
You can learn more about polyols and fructose in the articles: What Are Polyols? Learn All About the “P” in FODMAP! and Understanding Fructose Intolerance: A Lesser Known Dietary Trigger
Ok, onto the last “Layer”: Genetic Sucrase-isomaltase Deficiency
I mentioned way back there that it is possible for someone to have IBS-M and other conditions, or “layers” to their story, and I wish I knew about Genetic Sucrase Isomaltase Deficiency.
This condition occurs in approximately 30-35% of people with IBS-D (Irritable Bowel Syndrome with Diarrhea).
It often arises when individuals have certain genetic mutations or when their small intestine has been damaged, such as from conditions like Celiac Disease or Small Intestinal Bacterial Overgrowth (SIBO).
Yes, yes… I’m aware that this article is about IBS-M, and not IBS-D; but it can occur in those with IBS-M- though that figure is less established.
But if your random diarrhea episodes only come after having a candy party or if you link your diarrhea with specific foods that are high in sucrose or starch this could be a consideration after ruling out other common layers for IBS-M.
The biggest clues that indicate this issue include symptoms like bloating, gas, and loose bowel movements after consuming foods that contain a specific sugar known as sucrose.
This sugar is commonly found in sweets, baked goods, and even natural foods like carrots, garlic, and onions (hello FODMAP overlap!), as well as in starches such as rice, sourdough, bread, and grains.
For testing and treatment, samples of your small bowel can be collected using an endoscope, which is a camera that goes down your esophagus to examine your upper gastrointestinal tract.
These samples are then analyzed to assess the activity of the enzymes that typically break down sucrose and starch in the gut.
While there are medications and enzymes available for management, dietary modifications can be very effective, though they may be quite restrictive depending on an individual’s tolerance to sucrose and starch.
Whhhheeeewwwww! If you’ve read this far, I’m sending you a crisp high-five from Vancouver Canada.
The IBS-M Recap

I know that was a lot, so here’s a quick recap for you:
- IBS-M (Irritable Bowel Syndrome with mixed bowel habits) involves alternating between constipation and diarrhea, and accounts for about ⅓ of all cases of IBS
- IBS is now classified as a disorder of gut-brain interaction (DGBI), with symptoms linked to the gut-brain axis’s miscommunication
- Key symptoms include irregular gut motility, changes in gut microbiota, visceral hypersensitivity, and altered gut-brain signaling
- Diagnosis involves ruling out other conditions with tests and applying the Rome IV criteria, which focus on recurrent abdominal pain and changes in bowel habits
- IBS-M is diagnosed when more than 25% of bowel movements are loose or watery, and another 25% are hard or dry
- Effective treatment often includes working with a registered dietitian and may involve the Low FODMAP Diet to manage symptoms like bloating and abdominal pain
- Gut-directed hypnotherapy is highlighted as a promising treatment for addressing underlying issues in IBS-M
- IBS-M can also coexist with other conditions, such as histamine intolerance, sugar intolerance, or genetic issues like sucrase-isomaltase deficiency
- Medications, such as tricyclic antidepressants (TCAs), may help but can exacerbate constipation and have many side effects, so consultation with a doctor is important
- It’s crucial to tailor dietary and treatment strategies to individual needs, as IBS-M symptoms can vary significantly from person to person, so seek the support of your Doctor, and an RD whose practice is focused on IBS and related conditions
PS: Don’t forget your free IBS-M Guide here.
PPS: IBS-M is very treatable, so never give up advocating for yourself!
Stay well my IBS-M friend.
Resources:
- Amitriptyline at Low-Dose and Titrated for Irritable Bowel Syndrome as Second-Line Treatment in primary care (ATLANTIS): a randomised, double-blind, placebo-controlled, phase 3 trial
Ford, Alexander CFord, Alexander C. et al.
The Lancet, Volume 402, Issue 10414, 1773 – 1785 - Peters SL, Gibson PR, Halmos EP. Smartphone app-delivered gut-directed hypnotherapy improves symptoms of self-reported irritable bowel syndrome: A retrospective evaluation. Neurogastroenterol Motil. 2023 Apr;35(4):e14533. doi: 10.1111/nmo.14533. Epub 2023 Jan 20. PMID: 36661117.
- Lacy BE, Cangemi D, Vazquez-Roque M. Management of Chronic Abdominal Distension and Bloating. Clin Gastroenterol Hepatol. 2021 Feb;19(2):219-231.e1. doi: 10.1016/j.cgh.2020.03.056. Epub 2020 Apr 1. PMID: 32246999.
- Villanueva-Millan MJ, Leite G, Wang J, Morales W, Parodi G, Pimentel ML, Barlow GM, Mathur R, Rezaie A, Sanchez M, Ayyad S, Cohrs D, Chang C, Rashid M, Hosseini A, Fiorentino A, Weitsman S, Chuang B, Chang B, Pichetshote N, Pimentel M. Methanogens and Hydrogen Sulfide Producing Bacteria Guide Distinct Gut Microbe Profiles and Irritable Bowel Syndrome Subtypes. Am J Gastroenterol. 2022 Dec 1;117(12):2055-2066. doi: 10.14309/ajg.0000000000001997. Epub 2022 Sep 6. PMID: 36114762; PMCID: PMC9722381.
- Shah A, Ghoshal UC, Holtmann GJ. Unravelling the controversy with small intestinal bacterial overgrowth. Curr Opin Gastroenterol. 2023 May 1;39(3):211-218. doi: 10.1097/MOG.0000000000000928. Epub 2023 Mar 1. PMID: 37144539.
- Onana Ndong, P., Boutallaka, H., Marine-Barjoan, E., Ouizeman, D., Mroue, R., Anty, R., Vanbiervliet, G. and Piche, T. (2023), Prevalence of small intestinal bacterial overgrowth in irritable bowel syndrome (IBS): Correlating H2 or CH4 production with severity of IBS. JGH Open, 7: 311-320. https://doi.org/10.1002/jgh3.12899
- Lacy BE, Pimentel M, Brenner DM, Chey WD, Keefer LA, Long MD, Moshiree B. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. Am J Gastroenterol. 2021 Jan 1;116(1):17-44. doi: 10.14309/ajg.0000000000001036. PMID: 33315591.





